

IMS & SUM Hospital

AIIMS Raipur
What if a drug class developed for diabetes could also reshape how we manage inflammatory arthritis and rheumatic diseases? Since the approval of the first GLP-1 receptor agonist, Exenatide, in 2005, these agents have rapidly evolved—from glucose-lowering therapies to important strategies influencing weight loss, cardiovascular risk, and systemic inflammation. In parallel, our understanding of rheumatic diseases has also shifted. The obesity–inflammation axis is now recognized as a key driver of disease activity, treatment response, and long-term outcomes, especially in conditions such as osteoarthritis, psoriatic arthritis and in other inflammatory arthritides.
Patients with obesity often have more severe disease and respond less favorably to conventional therapies, highlighting an unmet need for strategies that address both metabolic and inflammatory pathways. GLP-1 receptor agonists are uniquely positioned at this intersection. GLP-1, an incretin hormone secreted post-prandially by intestinal L-cells, acts via receptors expressed in multiple tissues, including the pancreas, gastrointestinal tract, brain, adipose tissue, and skeletal muscle. These agents enhance glucose-dependent insulin secretion, suppress glucagon release, delay gastric emptying, and promote satiety through central pathways—thereby driving sustained weight loss.
Beyond these metabolic effects, GLP-1 receptor agonists also target the obesity–inflammation axis. Adipose tissue, far from being inert, functions as an active endocrine organ, releasing pro-inflammatory cytokines such as IL-1β and TNF-α, contributing to a state of chronic low-grade inflammation (“metaflammation”). By modulating this pathway, GLP-1 receptor agonists may exert both direct and indirect anti-inflammatory effects.
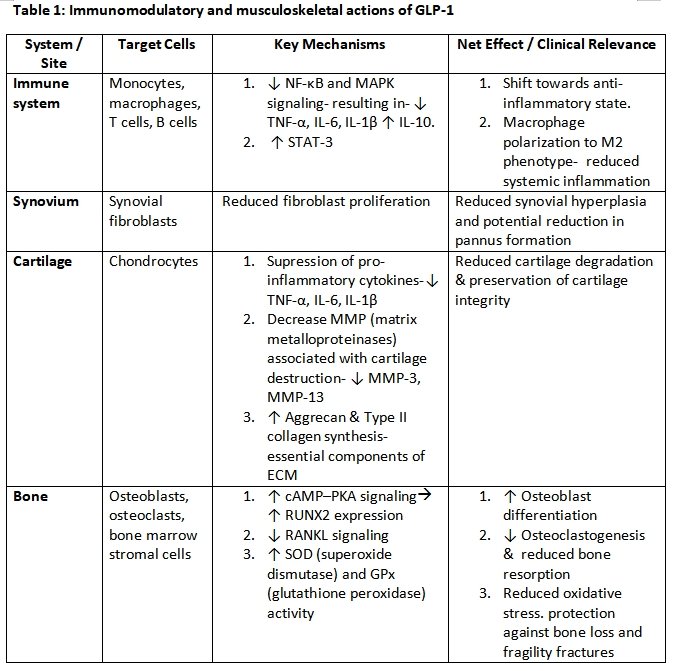
Accordingly, emerging evidence suggests that GLP-1 receptor agonists may have meaningful immunomodulatory and musculoskeletal effects, positioning them as promising adjuncts in the management of inflammatory rheumatic diseases. These are summarized in Table 1.
Building on these mechanistic pathways, a growing body of clinical evidence has begun to explore the role of GLP-1 RA in rheumatic diseases. The most compelling data currently emerge from studies in conditions such as osteoarthritis and psoriatic disease, where the impact of weight reduction and inflammation modulation is particularly pronounced. In a randomized, placebo-controlled trial (published in 2024, NEJM), once-weekly semaglutide in patients with obesity and knee osteoarthritis resulted in significant weight loss and clinically meaningful reductions in knee pain, along with improved physical function. The benefits were substantially greater than with lifestyle measures alone. In the recently published TOGETHER-PsA trial in obese patients of psoriatic arthritis, 31.7% of patients on combination therapy of ixekizumab plus tirzepatide achieved the primary endpoint of ACR50 response combined with >= 10% weight reduction, compared to only 0.8% with ixekizumab alone. In rheumatoid arthritis, retrospective data suggest improvements in disease activity and cardiovascular risk profiles. In addition, preclinical studies in mice & murine models of myositis and Sjögren’s disease respectively further support positive findings, with GLP-1 receptor agonists.
Despite these encouraging findings, some concerns remain. Data in systemic lupus erythematosus (SLE) are limited and somewhat conflicting. A Mendelian randomization analysis has suggested a potential association between GLP-1 receptor activation and expansion of IgD-CD27-double-negative B cells, which are linked to disease activity. In addition, isolated case reports have described adverse immune-mediated events, including leukocytoclastic vasculitis (LCV) and drug-induced lupus (DIL). Hence, In the context of inflammatory arthritis, GLP-1 RAs may offer considerable utility as adjunctive treatments, potentially augmenting the therapeutic efficacy of conventional DMARDs or biological agents, but this cannot be considered definitive based on the evidence so far provided. Notably, the role of GLP-1 RAs in vasculitis and vasculitic syndromes remains largely unexplored. As research evolves, GLP-1 RAs may emerge as a unique therapeutic bridge between metabolism and immunity—an area of growing relevance for modern rheumatology.
References
Copyright 2026 IRA eNewsLetter. All rights reserved. | Powered by BoxCloud


