Answer:
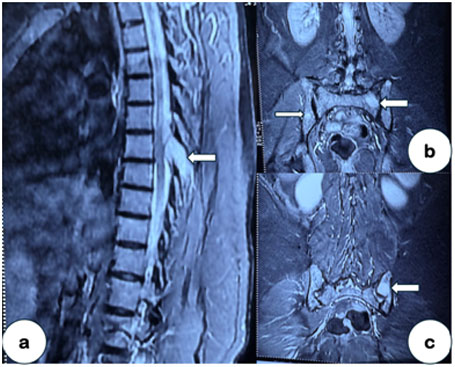
Multiple Myeloma with well-defined edematous lesions in the pedicle and the sacroiliac joint.
Figure a: Involvement of the pedicle, being enlarged on indenting the spinal cord.
Figure b & c: Multiple well-defined edematous lesions in the sacral and iliac part of the sacroiliac joint.
Further evaluation: Given night pain, elevated ESR and hypergammaglobulinemia, serum protein electrophoresis was also requested along with MRI, and she had a positive ‘M’ band.
Message: ‘All that glitters is not gold’. Low back pain that disturbs sleep is a red flag. Edematous lesions in the sacroiliac joint are not always inflammatory, even when inflammatory markers are elevated. We should always consider the differential diagnosis for inflammatory back pain, if any atypical features are present (middle-aged female, elevated ESR and hypergammaglobulinemia).