Psoriasis is an immune-mediated chronic inflammatory skin disease. It is easy to diagnose when silvery scales are seen on erythematous base usually affecting the scalp, elbows & knees, hands & feet, and shins. These are the friction/trauma sites that are affected the most.
Psoriatic arthritis (PsA) affects up to 30% patients with psoriasis. In approximately 19% patients, PsA symptoms develop before skin lesions. For a rheumatologist, when a patient of oligoarthritis presents with atypical skin lesions, it is important to be verse with uncommon skin lesions of psoriasis.
Inverse psoriasis affects the body flexures. Deep red colour of lesions, smooth skin surface with well-defined borders but without scales is diagnostic (Figs 1&2). The closest differential diagnosis is dermatophytosis of the flexures. Dermatophytic lesions are pruritic, asymmetric and have irregular advancing margins (Fig 3).
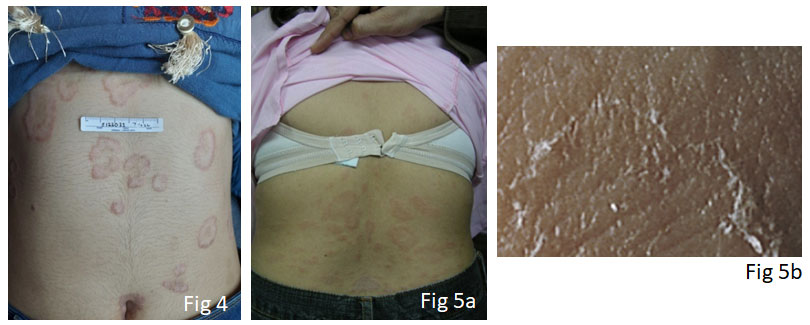
Annular psoriasis is another uncommon clinical expression of psoriasis (Fig 4). Lesions are erythematous with scaling at the border and central clearing. They closely resemble pityriasis rosea (Figs 5a & 5b), that presents with discrete oval lesions with inward looking collarette of scales, and this latter feature is diagnostic of pityriasis rosea.
Guttate psoriasis is a distinct variant seen in approximately 8% of psoriasis patients. The lesions are approximately 1 cm across, erythematous scaly tear-drop papules (Fig 6) widely spread over the body with maximum concentration over the trunk. The closest differential is pityriasis lichenoides chronica(Fig7) expressed as approximately 1 cm oval erythematous papules with brown hue and mica-like scale, wide-spread over the body with maximum concentration over the trunk.
Acrodermatitis continua of Hallopeau is a rare type of localized psoriasis typically limited to the tips of one or two fingers and toes (images can be seen at www.huidziekten.nl). Lesions are erythematous scaly with tiny pustules in the background. It tends to extend to involve the nails. The closest differential diagnoses are contact dermatitis, dermatophytic or bacterial infections.
In a patient with oligoarthritis with atypical skin lesions, skin biopsy can be instrumental in confirming the diagnosis.
Suggested Reading:
Yan BX, Chen XY, Ye LR, Chen JQ, Zheng M, Man XY. Cutaneous and Systemic Psoriasis: Classifications and Classification for the Distinction. Front Med (Lausanne). 2021 Oct 13;8:649408.
Kimmel GW, Lebwohl M. Psoriasis: Overview and Diagnosis. Evidence-Based Psoriasis. 2018 Jul 1:1–16.